
I recently had the opportunity to sit down with Pete McCanna, the CEO of DFW-based Baylor Scott and White, one of the, if not the best-run health system in the country. Pete was gracious enough to spend more than an hour with me discussing leadership, Baylor’s health system transformation strategy, thoughts on physician alignment, jobs to be done in healthcare, and innovation. I’ve summarized the main takeaways below and I hope you guys enjoy because I personally loved this conversation. Lots of practical takeaways from a great person. We uhh…talked a LOT.
Let’s dive in!
PS – Join my Hospitalogy Membership! If you’re a VP or Director working in strategy or corporate development at a hospital, health system or provider organization, you will get a lot of value out of my community as I purpose-build the content, fireside chats, and conversations for this group. Join for free today.
Baylor’s Health System Transformation Journey: Moving from Healthcare 1.0 to Healthcare 2.0
Most health systems are stuck in healthcare 1.0 today.
Historically a normal hospital CEO – by the book – focuses on his or her hospital’s asset utilization, and how that utilization’s translates into good financial performance, better quality performance, and solid patient survey results. This healthcare 1.0 thought process was (and remains) the traditional way of thinking at most hospitals prior to the big health system transformation push. Thoughts like these pervade hospitals and health systems across the country:
- What assets do I have to work with? What service lines should I focus on?
- How do I implement tactics upstream that get me utilization in those desired service lines?
- What other levers can I pull to acquire customers (patients) at all costs? I think I’ll acquire that medical group. Or I’ll leverage my rates or ask for higher prices or whatever lever is at the hospital’s disposal to move the financial and operating needle.
But for Baylor, in this state of healthcare, a pressing question still nags: how is this model any better for the customer? And the answer is…it isn’t.
So, with those past lessons in mind, Pete and Baylor are slowly inverting the traditional health system model. Baylor is 3 years into their health system transformation strategy and starting to see the fruits of those efforts in 2025.
How? By doing right by their customer.
In doing so, Baylor had to focus on long-term strategic pivots, and it wasn’t easy. And as part of this transformation journey, Baylor is completely up-ending the traditional health system heads in beds model, flipping from a supply-driven healthcare system…to a consumer-oriented, demand-driven one.
For Baylor, Healthcare 2.0 Involves Relentless Pursuit of the Customer
“If we win, and if our strategy plays out like we expect, we will help transform healthcare. We will be an early mover from a healthcare system that has historically been supply side driven into one that is driven by demand. One that is designed based upon you as a customer as opposed to the old design based on health systems with assets optimized for utilization of these assets – heads in beds.”
Instead of having that legacy healthcare 1.0 system focused on being incrementally better over time, Baylor wants to move to healthcare 2.0, and solve problems for patients who come through its doors. By doing that, the rest will fall into place. They’ll acquire customers by gaining loyalty in pursuit of excellent patient care, iterating, and continuing to pursue the customer.
The crazy thing is…solving customer problems is not a novel idea. In fact, it’s what other businesses in other industries do in order to compete and make money. It’s what health tech startups aim to do by recognizing rampant problems in our broken healthcare system. And it’s now what Baylor has embarked on.
As far as disruption is concerned, Pete believes the transformation of healthcare will happen from the inside out. Not that those outside looking in won’t participate and help with the transformation, but simply that the level of complexity and walled garden nature of the healthcare system necessitates being on the ‘inside’ to drive meaningful change. from those who have the assets and long-term, community-driven mission to local populations.
In talking to Pete, it was clear that point solutions contribute to the healthcare fragmentation and connectivity problem, leading to worse patient experience. Point solutions are trying to penetrate the healthcare system, but they just hit the system and then eventually fall off. There’s no integration, no downstream follow-up, just further fragmentation – similar to what happened with retail health. No connectivity to the rest of the healthcare system and appropriate navigation of patients to the right care setting. They create a disjointed experience, leading to frustration.
Baylor’s Consumer-Facing Products
Still, there’s more competition than ever across digital health and outpatient care. So Baylor set out to prioritize products and service lines based on its own customer research, data, and leveraged the 80/20 rule in development: “what’s the best bang for our buck we can invest in as a health system to deliver the most value to our patients? What do customers really want?”
Here’s much of what Baylor identified and launched:
First Contact Navigation:
Patient navigation was an obvious first choice given rampant need both organizationally at Baylor but also to empower their consumers and prevent network leakage at the health system. Pete holds intense conviction that solving patient navigation, access, personalization, and convenience is paramount to Baylor’s consumer-centric strategy. It was a no-brainer to start here. Baylor’s First Contact navigation app is described simply, but complex logistically. From the user side, a patient enters symptoms. Then engages in a chatbot discussion. Later on, the patient has option to speak to human being if they need to. By the end of 5-8 interaction, the patient gets scheduled with the right Baylor provider or finds the right care setting.
In developing the First Contact app, Baylor conducted quite a bit of research, applying consumer business principles and looked at consumer journeys. In other words, Baylor asked themselves “what is the typical consumer journey here, and how do we reimagine that journey, and synchronize the care?”
“If we get that right – navigation, expand the ecosystem with more choices, and synchronize the patient journey, that the patient will be more delighted, and most importantly, you’ll have better outcomes over time.” More touchpoints lead to better outcomes.
In one of its trial runs, Baylor researchers asked the participants “if you didn’t have our navigation tool, where would have you gone?” 60% of the respondents responded that they would have picked a different location, and generally this pick would have resulted in a a higher cost, higher acuity location. Marinate on that point for a second. SIXTY percent of the people flowing through healthcare systems are entering the system at the wrong place. As Pete described it (and I think it’s pretty apt), it’s like going to buy an F-150 and ending up with a Ford Taurus.
Baylor re-routed something like 80% of patients who WERE going to go to the ED to urgent care or virtual visits. And so as Baylor’s demand for services shifted, and as the organization moves over time from supply-driven to demand-driven, that means Baylor’s supply side – their asset base – needs to respond. Now, instead of building solely for supply, Baylor’s healthcare asset additions relate to what customers want, and they have the data to understand those patterns.
This dynamic is also driving Baylor’s M&A strategy. For instance, Baylor purchased 41 urgent cares in mid 2023, looking to add even more access – and it’s totally driven by what the consumer wants. We as consumers want care now, and we want it to be convenient. And this dynamic is also where a huge advantage presents itself on the health system side and the inside-out nature of healthcare 2.0 transformation. When Baylor acquires an urgent care center, it’s not a point solution. It’s integrated into the rest of their system. What’s the on-ramp for a Baylor patient to its urgent care, then the rest of the system? It’s through the app, which builds loyalty and reinforces customer behavior. You can schedule an appointment at urgent care or add yourself to the line, and then what’s the off-ramp for that patient? Do you have a PCP? If not, Baylor will connect you with one. Do you have a follow-up visit scheduled? They’ll add it to your calendar. Connected care. Boom. Once the patient experiences this, they won’t go elsewhere. It creates a premium walled-garden experience, and Baylor is not alone in engaging with this trend.
Here’s a cool example straight from Pete himself. Pete’s family member had a back problem which turned out to be a tear in her shoulder. In healthcare 1.0, the cumbersome process would have involved going to the PCP first, waiting a few weeks to do so, at which point the PCP would confirm a problem, order some imaging, get the report, then refer to an orthopod. If you’re lucky in this healthcare 1.0 scenario, you’re 8 to 10 weeks out from a fix to your problem. And ALSO if you’re lucky, you’re properly diagnosed.
Under Baylor’s model, Pete’s family member had the problem fixed in a week. Within 24 hours they had seen a specialized APP who works in muscle and joint care chatting, received a full symptom list, ordered imaging, received that imaging within 24 hours, then 24 hours after that saw a pain specialist. The pain specialist noticed a more nuanced problem and ordered an MRI. Within 24 hours they had THAT done, and the specialists found a tear in her tendon. Within 8 days, his family member had surgery scheduled to fix the problem. THIS is healthcare 2.0, and it’s the future Baylor is striving toward.
‘Specialized’ Primary Care:
Pete and I chatted a bit about specialized service lines where patients can get direct access to care for nuanced, yet repeated conditions. Certain service lines or conditions where people have chronic conditions but have trouble getting relief or appropriate care for. Pete used the example of chronic headaches. For chronic headaches, in the old healthcare model, the patient would go to the PCP and would leave frustrated. Then they would go to the neurologist and cause frustration for the specialist given how low acuity the condition was. In Baylor’s new model, they’ve set up virtual care visits for headaches specifically, then follow-up care from headache specialists, and prescriptions, and so forth – with access to this care 24/7. Think of it as specialized primary care, in a sense.
Women’s Health:
Baylor has built out its own proprietary women’s health concierge model. The first version of this service line was 24/7 post-partum care. It since has expanded into full spectrum women’s health care – where the new model of care fills in the gaps between appointments to help women feel supported and cared for during their birth journey – not too dissimilar from other women’s health startup concierge models in the wild.
Behavioral health:
Baylor also identified behavioral health as an area of sore need and is in the process of building a behavioral health product. More to come on this, I’m sure!
Longitude Health:
Alongside these internal Baylor initiatives, Baylor has also partnered with other large nonprofit health systems on an innovation engine called Longitude Health. Since launching, Longitude Health has formed three companies in the realms of value-based specialty care, revenue cycle management and financial experience, and finally, specialty pharmacy.
Baylor’s 3-Year Journey, and Expectations for 2025 and Beyond
I asked Pete next about how Baylor’s grand strategy came together over the past few years along with where Baylor is headed in 2025+.
2023 was where Baylor’s current strategy was conceptualized. During 2023, many health systems were slowly re-emerging from the pandemic and dealt with labor, supply, and utilization woes, but that last tide was turning. Baylor in particular is situated in good markets demographically and runs has a tight operating model, organized in such a way that they could be nimble and flexible around their local markets when the environment shifted. In the back half of 2023, utilization returned and the environment shifted to more favorable conditions for health systems. Still, as Baylor’s local Texas markets returned to more ‘normal’ operating environments, Baylor had to stay on its toes. It competes against heavy hitters in Texas, including the likes of systems like HCA, Tenet, etc.
Baylor started gaining traction on its new transformation strategy in 2024, but it also had to deal with growth and capacity constraint. Populations within Baylor’s markets swelled in 2024, and the compounding effect of the return of utilization was a double whammy, leaving organizations scrambling to match supply and capacity with newfound demand. So capacity management grew to be top of mind, and Pete mentioned Baylor taking two approaches to it. In the short term, Baylor launched dozens of tactics to address issues in the short term while at the same time thinking about ways to future proof capacity management in the long term.
What’s nice about Baylor’s current strategy is that doing the hard work around business model transformation also solves for capacity management over a long-term horizon. Tools like patient navigation are designed to help their customers in getting patients to the appropriate care setting at the right time, but they’re also helpful to Baylor on the back end to manage its service lines and asset bases. By adding outlets and virtual and urgent care, it alleviates capacity management. Baylor also added beds across its portfolio (Roundrock, Waxahachie, Frisco) to match up with population trends – the organization doesn’t see the growth stopping in its local markets any time soon. A great problem to have!
Also in 2024, Baylor launched version 8 of its app. Most health systems say they have an app, but it’s really MyChart with maybe a few bells and whistles. Baylor’s has been in development for a while, and 80 to 90% of its contents are non-Epic or EHR related. A core pillar of Baylor’s strategy is that if consumerism is going to enter healthcare just like it’s entering every other industry, then Baylor HAS to have a top-notch customer engagement platform – and that’s Baylor’s app. It functions as a hub for supply management, demand management, virtual care delivery. So in v8, Baylor added 100+ new features in 2024.
So while Baylor is adding capacity and continuing legacy system operations (which are still important), Baylor will continue this pivot to customer centricity. The plan is that we’ll look up in 3 to 5 years, and Baylor will be significantly differentiated as a health system from its competition.
On the policy side of the equation, Pete anticipates ongoing federal policy impacts, particularly around 340B and site-neutral payments. Baylor thinks it’s very well positioned for site-neutral payments, because Baylor implemented a joint-venture ambulatory strategy a long while ago with ASCs, rehab, and the like. Baylor was very forward thinking in that way. Notably, Pete mentioned It’s hard to fight site neutral policy. Price differentials are double in most systems. Pete is of the mindset that we ought to embrace it – almost out of necessity, since acuity is rising, health systems are pushing things into the outpatient setting as inpatient admissions grow in complexity.
Looking toward 2025, Pete emphasized continued execution on Baylor’s customer-centric approach including enhancements to the patient journey, touchless check-ins, streamlined payment experiences, digital platform investments, new product solutions (e.g., behavioral health), and strategic efficiency amid growth. There will always be a gap between price growth and expense growth, and Baylor has to deal with that. Finally…Baylor and everyone else will be trying to figure out what’s going to come out of Washington.
Baylor’s Feedback Loop and Jobs to be Done
Pete detailed Baylor’s rigorous feedback mechanisms – consumer surveys, traffic analysis, focus groups, home observations, and human-centered design methods – to continuously refine products and services. For instance, Baylor hired people who have done human-centered design to ask consumer-facing questions like “Do people prefer this tab or that color, this color or that, or to get to this feature how many clicks do you need to make?” If you have a clunky app it’s a horrible experience and so that becomes an important piece.
Key “jobs to be done” in the near future, as part of the grand strategy, include eliminating customer friction, enhancing digital engagement, ensuring effective patient navigation, proactively closing care loops, and diligently managing patient access to prevent potential customers from being turned away – a problem often overlooked by traditional healthcare systems.
I thought this was a particularly interesting point. In discussing this dynamic, Pete mentioned a Home Depot study, and compared it to healthcare. In that study, Home Depot realized that there was a large percentage of people who entered their stores, had a list of things to get, yet left empty-handed because they couldn’t find what they were looking for. What a headache for a business. In healthcare, it’s similar. We have demand we can’t satisfy. People try to go on Baylor’s website, or call a contact center, or try to schedule a follow up, and they get lost along the way and don’t reach their ultimate destination.
Overall Baylor believes it has a 3 year lead on competition, and if they continue to put the customer at the epicenter it’ll only serve to differentiate their organization over time.
Baylor’s Physician Strategy with HTPN
A more nuanced line of questioning I asked Pete related to Baylor’s physician alignment strategy—specifically, what’s going on in Baylor’s markets, his thoughts on the current state of the subsidy model (which has been characterized as unsustainable), and which approaches work in which market. Here were some takeaways:
Every market is different for a health system, and different tactics are needed in each. However, there’s one constant: you need to have a critical mass of physicians—a comprehensive, employed medical group with strong specialty coverage. And if you operate a fully integrated platform, you can—and should—also include independent physicians within that network.
Having this asset is vital for several reasons:
- Baylor can credibly deliver on a risk-based relationship with an employer or payor and bring the full continuum of care—with uniform standards within Baylor’s ecosystem—without relying on anyone else.
- The physician or professional entity serves as an innovation center: a place where Baylor can launch new products and services, refine and iterate on them, and then scale them to the rest of the enterprise once perfected. Often, the employed physician base leads health system innovation. Having that capability within Baylor’s employed group is important.
- The organization acts as a training ground for great leadership, in the long term. Many senior physician leaders at Baylor have risen through the employed group and distinguished themselves. In Baylor’s model, physician leaders eventually reach a point where they run a sector of the business. Pete specifically mentioned a surgeon in Austin who is now the EVP helping to run the entire delivery system in Baylor’s dyad leadership model.
Physician Employment and Subsidy Model – What’s the Outlook, and Is It Sustainable?
Ultimately, whether your physician alignment model works comes down to where the value creation lies. Ask yourself: what’s the job to be done? For instance, acquisitions and consolidation of physician practices make sense if you can draw a clear line to the patient and demonstrate how you improve patient care. They generally don’t work long term if you’re engaging in financial engineering or arbitrage, which is why we saw some of the PPMs falter over the past few years.
With the various physician employment models, the biggest question is…what KIND of value are you creating? And why is that health system—or PE or other consolidator—employing physicians? Is it to arbitrage rates? That type of financial engineering and ‘non-value’ creation is going to disappear.
The question is whether there are employment models that lead to genuine value for the customer and whether those models are economically feasible. Take risk management as an example. If you can create a model of care through a tighter relationship—for instance, using senior-only clinics—patients generally appreciate it. They’re getting more access; some even receive 12 or more touchpoints per year.
DTC specialty care is a new trend. It’s unstoppable. In certain conditions, consumers will be armed with enough knowledge about their own conditions—using AI and similar tools—so that they want to go straight to the specialist.
Provider-Sponsored Plans: What Do These Unlock for Baylor, and Are They Viable?
Notably, provider-sponsored plans scaled back from Medicare Advantage (MA) in 2025 and lost considerable market share. For Baylor, however, Pete mentioned a couple of key roles these plans play as part of an overall enterprise strategy. In certain markets (e.g., central Texas), having an insurance entity that collects premiums provides a model that helps Baylor operate a closed-loop system—especially in government segments (Medicare, Medicaid). This is a perfect example of why local market differences matter. For instance, demographically, the population in central Texas sees less turnover.
On the Medicare Advantage side, when Baylor holds a critical mass of providers in a certain geography, they can launch an MA plan in lieu of working with carriers.
Finally, for self-employed large employers—working in conjunction with Baylor’s ACO, Health Plan, and app—Baylor can customize an array of products and services catered to employers. Baylor offers a portfolio of solutions that covers all the major needs of these organizations, all integrated into an app, giving Baylor the ability to assume employer risk.
At a high level, although it’s not exactly a money-printing machine, the risk-based part of Baylor’s business supports the overall, system-wide strategy. Increasingly (and notably), Baylor believes its health plan needs to become a platform experience as well, and the advantage is that they can control that trajectory. In general, healthcare is moving toward platforms over time.
Pete’s final strong point on provider-sponsored plans centered around the challenges they face against savvy competitors. By definition, provider-sponsored plans are subscale. This regional dynamic means that larger national plans will always be more efficient than you. So the question is…how can you create scale—not only in density but also in capability through AI, data, and other necessary components for managing risk? The answer is…through collaboration. To that end, Baylor is working with Longitude Health to develop a population health platform. This nationally scaled solution can then be sold to subscale plans to share the benefits of scale without needing to be a national player. An interesting, notable little venture.
Local Market Dynamics Matter
One more note on the power of local market dynamics to drive the point home:
Baylor’s markets have nuances that affect its strategy in each particular area. While Baylor’s overall enterprise strategy and core customer-centric theme remain the same, each market requires different tactics to achieve the best results. For example, Austin is distinct from Temple or College Station. In Austin, while Baylor might not be the largest player by market share, the organization holds the largest employed physician group in the city. With that crucial asset, Baylor is carving out a niche with more flexibility and nimbleness than, say, HCA or Ascension. Even as they build out their Austin presence, the shift toward health system transformation (rather than old-school tactics) is clear, and their integrated offering will grow over time.
Moving to Central Texas and Temple, Baylor holds a 75% market share, and there’s much more government reimbursement, so taking on Medicaid or Medicare risk makes sense—they dominate these areas.
Finally, in DFW (!!), health plans don’t play as significant a role, but ACOs take precedence. Physician dynamics in DFW lean more toward independent private practices. According to Pete, half of DFW physicians are either in private practice or not affiliated with a health system, making tight integration in Dallas more challenging. On the commercial side, DFW is an open-choice market, so taking on commercial risk isn’t as viable.
These are just a few examples of market nuances in Texas alone. Now, imagine scaling that to hundreds of MSAs across the country, across health systems, payors, and every healthcare services organization in between!!
Baylor and Innovation in AI
Of course, I had to ask Pete about AI in healthcare and how he sees Baylor leveraging it across the organization. Baylor is a big believer in AI—but the big question is “how do you adopt it?” Pete described AI as akin to throwing rocket fuel on their customer-centric approach because AI is at ALL of our fingertips, equipping patients with more knowledge.
For instance, during a sprint review, Baylor identified a pain point: people get their lab results but don’t know what they mean, so they have to wait for the doctor. Now, patients can upload lab results to an AI system (with de-identified data fed into an LLM) to get an extensive evaluation of possible explanations for abnormal values. AI also turbocharges Baylor’s virtual tools and further empowers patients. Today, patients have access to much more information than they did even five years ago.
I can personally attest to these capabilities. When my son had some gut issues, I uploaded his results to ChatGPT and was able to understand what all the various bacteria levels meant. Pretty cool—and very empowering from a consumer perspective. On the flip side, as an administrator or physician, you must assume that every patient you meet may have already run their symptoms or lab results through ChatGPT. This dynamic is entirely new and demands better communication with patients to maintain trust.
The scope of healthcare is so vast because of its labor-intensive nature, and AI will eventually be infused into everything in the field. As with other product developments, Baylor is assessing every area and asking, “What’s the application of AI in this environment?” In 2024, Pete met with OpenAI and several other health system and payor executives, and he was stunned by some of AI’s capabilities—such as differential diagnosis—so he’s excited for the future on both the administrative and clinical sides. He even thinks AI will totally change primary care; the PCP will oversee AI and care teams over a much larger panel of patients, helping bolster access. That’s pretty cool.
Pete broke down AI solutions into three buckets:
- Individual use cases. In a protected enterprise environment, can Baylor provide you with your own personal assistant to use within certain parameters? For example, it can help with marketing press releases, legal drafts, or personal workflows. You can generate these outputs almost instantly rather than waiting for someone to type up a template. (I use it for that purpose too—even though it STILL sometimes hallucinates…sigh.)
- New and existing cases of AI.
- We’re seeing a revamp of legacy systems that are now infused with AI. For instance, in imaging: if a radiologist is working through his queue and someone enters the ED, AI can read the image before the radiologist does, triage certain images by flagging potential critical findings, and alert the doctor to stop the queue and review a critical image. With a smart system handling triage, the process is much faster and significantly impacts patient outcomes and ED throughput.
- In Pete’s view, it’ll be malpractice NOT to use AI-assisted tools because they’ll be that effective. I share this viewpoint. While many focus on the safety, compliance, and responsibility of AI—what I liken to the ‘self-driving car’ problem in healthcare (self-driving cars are statistically safer than human drivers, yet every crash makes headlines)—guardrails are important, but we should be pushing AI forward as much as possible, responsibly.
- AI-native solutions: Pete specifically highlighted AI’s translation capabilities (given that health systems spend millions on translation systems) along with agentic AI performing redundant tasks in areas like HR benefits, legal, and patient intake. For example, AI can listen to thousands of conversations to identify common issues and solve patient problems without direct human intervention—the list goes on.
- We’re seeing a revamp of legacy systems that are now infused with AI. For instance, in imaging: if a radiologist is working through his queue and someone enters the ED, AI can read the image before the radiologist does, triage certain images by flagging potential critical findings, and alert the doctor to stop the queue and review a critical image. With a smart system handling triage, the process is much faster and significantly impacts patient outcomes and ED throughput.
- Co-development. Baylor is developing new products (such as navigation tools) and is open to partnering with outside companies to infuse these products with an AI-enabled feature set.
The biggest force in AI and innovation right now is the velocity of change. Technological improvements are occurring so quickly that major changes can be seen every 60–90 days, which keeps upping the stakes for everyone involved (and even significantly affects the pricing of AI solutions). It’s truly exciting to see it all unfold in real time.
Talking Leadership with Pete
When I initially sat down with Pete, our first conversation was around why he became a leader in healthcare. For Pete, leadership is deeply personal. He believes healthcare has a huge potential to impact social justice positively, making a real difference in people’s lives.
The “Why” Behind Pete’s Leadership
This sense of purpose grew even stronger through his personal experiences – his mother struggled with chronic disease, and his father battled Parkinson’s. These close encounters showed him just how fragmented and difficult navigating healthcare can be, especially for families managing multiple health conditions.
Pete vividly remembers how his dad started giving him lists of issues to address, a habit that slowly transformed into Pete’s own life mission – a list he’s determined Baylor will tackle head-on. For Pete, healthcare’s brokenness is something leaders must actively fix, and he’s committed to making that happen.
Throughout these personal experiences, Pet was exposed to how broken our healthcare system is. He always knew it, but it’s hard to know how much so when you’re on the outside looking in. But when Pete was thrust into the balkanization of healthcare, he saw how really healthcare inflicts suffering on patients during the times between appointments, particularly for people with multiple conditions and the ability for family members to navigate the system on their loved ones’ behalf.
He strongly believes we now have the tools needed to shift healthcare from a reactive, paternalistic model to one that’s proactive and patient-centered, empowering individuals to manage their own health.
Pete sees leadership in healthcare as an opportunity to significantly impact community well-being, building strong, responsive organizations that truly improve people’s lives. In general, healthcare is in sore need of strong leadership from the front calling out the issues described above, and more.
How to Lead People at a Health System
Moving on to the “how” of leadership, Pete gave some great practical advice.
Clarity is essential when leading people in a complex organization like Baylor Scott & White. Be crystal clear on the “what” – the outcomes you want to get. For instance, ask yourself – what is the object and mission of all the activity of Baylor Scott & White?
Defining precise outcomes and aligning every action with delivering measurable benefits to patients and consumers is equally important in developing a consumer-centric, agile model. According to Pete, it’s crucial to adopt a rigorous, analytic approach supported by customer insights and scientific methodologies.
- Be radically customer-centric and constantly ask questions for the team: “what did we do for the customer that’s tangible and addresses their pain points?”
Create a framework or operating model for how your team operates. Then, within that framework, give teammates freedom to innovate with tools. This framework allows teams to innovate and proactively respond to patient needs, transforming healthcare from a reactive, paternalistic model to one that empowers individual participation.
Building an Effective Team
Pete candidly shared how his approach to team-building evolved over time.
Initially, he thought simply hiring top talent and giving them autonomy would ensure success. “I thought all you needed to do was hire the Blake Madden’s and Jonny Cantwell’s of the world, and we’d get it done.” (really tooting my horn there, thanks Pete).
But this thinking fell apart, and there’s way more nuance involved with team building than pure talent. Just ask any football coach. Pete came to realize that while talent is essential, cultural fit and alignment are equally, if not MORE critical. In thinking of potential leaders and team members on an axis, you need to put together teammates who have both (1) excellent performance and a great track record, and (2) the right fit and behavior.
A high-performing team member who doesn’t mesh well culturally severely impacts team effectiveness. As Kevin Durant and many others put it, “hard work beats talent when talent doesn’t work hard.” Today, Pete prioritizes team members who not only meet performance benchmarks but also align deeply with organizational values and culture, fostering cohesive teamwork. He’d take a mediocre (but still adequate from a benchmark perspective) performer with high fit over a good performer with bad fit for the team. That’s how important fit, culture, and behavior is to any organization’s success.
Leadership Cultivation at Baylor
In Part 2 I mentioned already how Baylor’s physician alignment and leadership development strategy has led to fantastic physician leaders throughout the organization. Here’s a few more thoughts on how Baylor identifies and develops leadership organization-wide.
In cultivating leadership at Baylor Scott & White, Pete focuses on intangible qualities such as energy, enthusiasm, and alignment with the organization’s vision. He explained the importance of finding leaders who see their roles as contributing to something genuinely meaningful and impactful beyond financial rewards. Money isn’t a primary motivator – there’s an additional push there in the sense that you believe in what you’re set out to do – and it’s on Pete to set that vision toward a true purpose of consequence. That they see their jobs as contributing to something of consequence is extremely important to accomplish in healthcare.
Intriguingly, Baylor also seeks talent outside the healthcare industry, particularly individuals experienced in digital innovation, to bring fresh perspectives. Pete firmly believes that effective leaders are driven by a deeper sense of purpose, knowing that their work directly contributes to significant, meaningful change.
Wrapping up with Pete McCanna and Baylor
While I don’t cover intangible elements of healthcare often, nor am I an expert in leadership and management, I always find the topic fascinating given how much work and effort goes into setting the vision for an entire organization like Baylor Scott & White.
I learned a lot from my conversation with Pete across leadership, Baylor’s consumer-centric strategy, and the economics at play in their various markets. Pete’s leadership philosophy integrates personal purpose, clarity of vision, strategic team-building, and cultivating a culture of purpose-driven leaders to create lasting improvements in healthcare. I hope Baylor succeeds in their health system transformation journey to a consumer-centric future.
About Pete McCanna
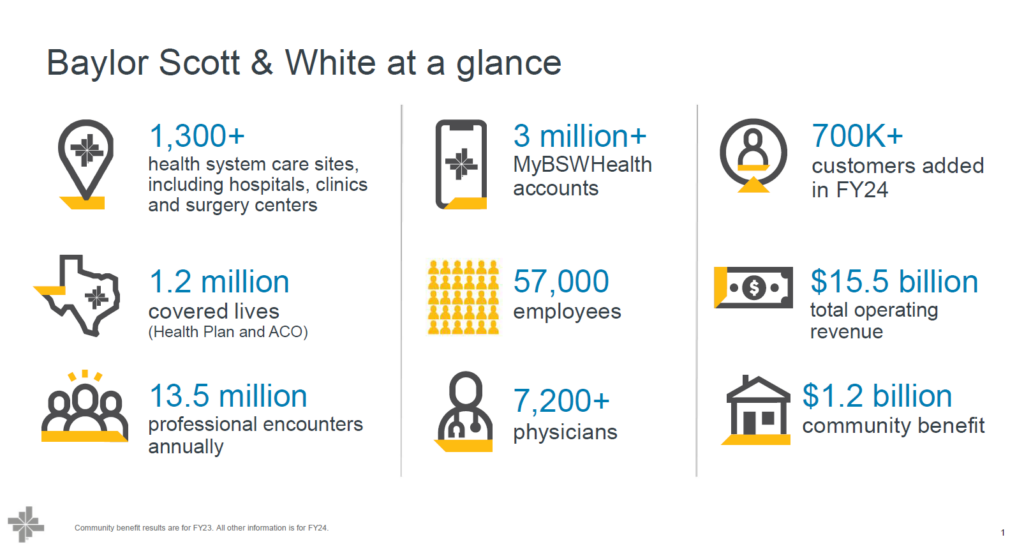
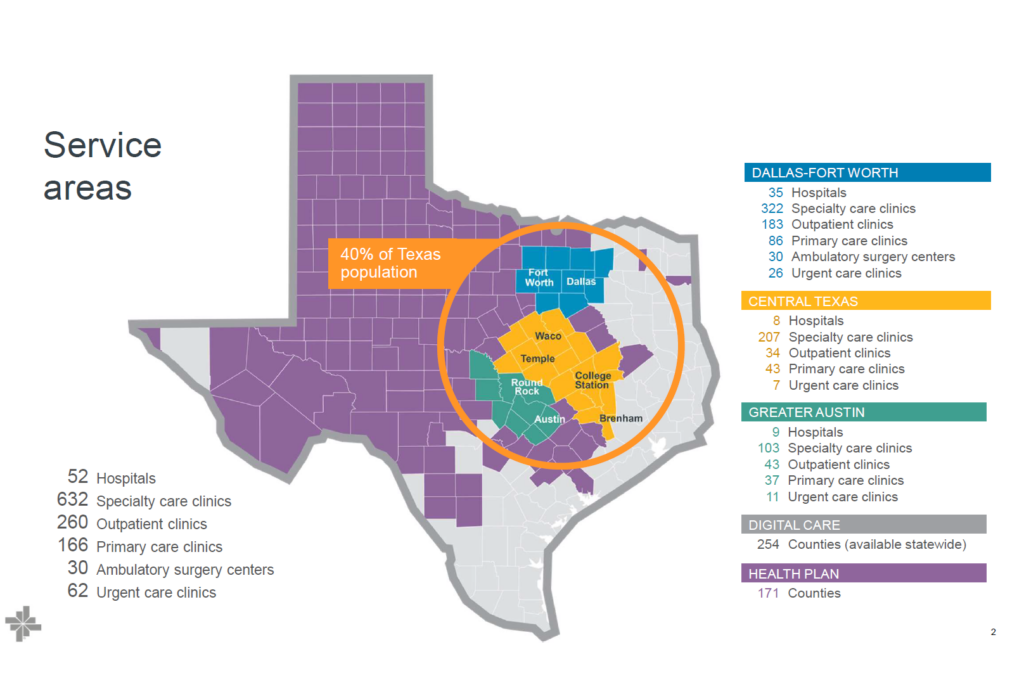
Pete McCanna is chief executive officer (CEO) at Baylor Scott & White Health, the largest not-for-profit health system in Texas. The system’s integrated delivery network includes Baylor Scott & White Health Plan, Baylor Scott & White Research Institute, Baylor Scott & White Quality Alliance, and its leading digital health platform, MyBSWHealth. Through 52 hospitals and more than 1,200 access points, including flagship academic medical centers in Dallas, Fort Worth, and Temple, the system offers the full continuum of care, from primary to award-winning specialty care, as well as an array of virtual and in-home services.*
As CEO, McCanna leads the health system’s transformation to deliver experiences that go beyond customers’ traditional expectations of healthcare. Before becoming CEO, he served as Baylor Scott & White’s president, where he advanced clinical alignment, accelerated the development of its digital health strategy, and expanded academic affiliations to help address the critical need for clinicians in Texas.
Previously, McCanna served as executive vice president and chief operating officer at Northwestern Medicine. During his tenure, operating revenue, quality, patient experience, and employee engagement exceeded targets. He was instrumental in Northwestern’s expansion as it maintained its AA+ bond rating.
McCanna has nearly 40 years of experience in healthcare management and consulting. Prior to Northwestern, he served as chief financial officer (CFO) at Presbyterian Healthcare Services and CFO at the University of Colorado Hospital. Earlier in his career, he worked for Denver Health and as a healthcare consultant for The Lewin Group.
Named by Modern Healthcare as one of the “100 Most Influential People in Healthcare” in 2024, he is the inaugural board chairman of Longitude Health, an innovative healthcare collaborative. McCanna also serves on the boards of University of Michigan Health, the Texas Hospital Association, and Catholic Extension. He holds a master’s degree from the Lyndon B. Johnson School of Public Affairs at the University of Texas at Austin and a bachelor’s degree in English from the University of Michigan.
PS – Join my Hospitalogy Membership! If you’re a VP or Director working in strategy or corporate development at a hospital, health system or provider organization, you will get a lot of value out of my community as I purpose-build the content, fireside chats, and conversations for this group. Join for free today.