
Why fragmented patient data became a financial and regulatory liability, and how clinical AI closes the gap at the point of care
TL;DR
- Fragmented patient data is now a liability, not a back-office annoyance. With V28 squeezing codes, RADV activity intensifying, and OIG and DOJ circling MA risk adjustment, retrospective chart chasing is how you get flagged, audited, and sued for overcoding.
- Navina closes the gap at the point of care, where medicine and money both get decided. Their solution reconciles EHR, claims, HIE, labs, notes, PDFs, and now ambient conversation into one patient picture inside the workflow, with every suggestion tied to source evidence.
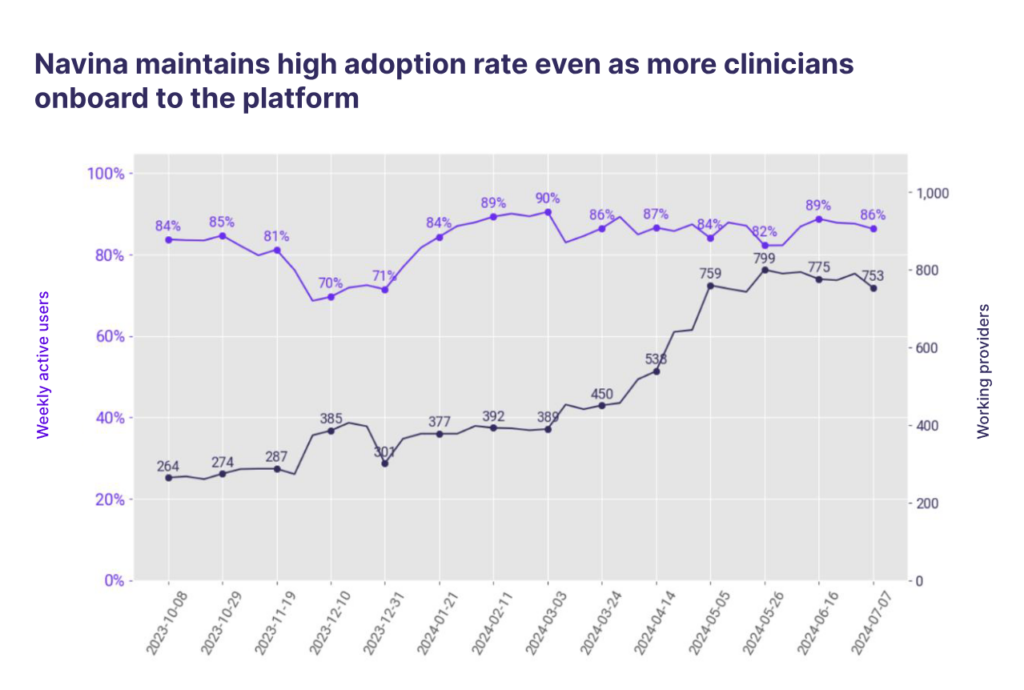
- ROI shows up as massive adoption. 86% weekly active providers, a 77% acceptance rate against ~40% in competitor case studies, 40% less chart-review time, and a +0.153 RAF lift across 3,100+ physicians in an independent, AAFP-affiliated study.
Healthcare’s data isn’t missing. It’s everywhere.
We talk about value-based care like it’s a contracting problem. Get the attribution and quality measures right, and performance follows. But the real work of winning under risk happens inside a 15-minute visit, with a physician rebuilding a patient’s story from records scattered across the EHR, an HIE, a claims feed, a lab portal, a specialist’s PDF three systems over, and a hospitalization nobody told the practice about.
None of that data is missing. It’s just smeared across a dozen disconnected sources with no single source of truth, which makes the clinician the integration layer. They piece the story together by hand, backtracking through tabs while the patient waits.
Think about all of the lost efficiency from this fragmentation. Physicians burn time they don’t have tracking random metrics down. Care gaps slip through because they’re buried in records nobody had time to read. Coding, quality, and care teams each work off their own worklist, generating handoffs and waste. And risk adjustment suffers when documentation doesn’t reflect a patient’s true complexity, which in 2026 is a compliance exposure on top of a revenue one.
This need for clean, consolidated data – used by the physician or clinician at the point of care – is a core piece of missing infrastructure so many provider organizations lack.
The cleanup-crew model is dead
For years, VBC documentation ran on retrospective cleanup: year-end chart chases and coding sweeps, recapturing conditions long after the visit was a distant memory. That model is now…a relic.
V28 is squeezing margins while RADV activity keeps intensifying. ACO REACH and the LEAD Model (launching January 2027) are raising the bar on documentation integrity. And the enforcement drumbeat only continues to exacerbate, with OIG and DOJ scrutiny of MA risk adjustment turning into a steady news cycle, including a recent OIG action on acute-stroke coding and a run of high-dollar settlements over diagnoses submitted without evidence.
An indefensible code is exactly what gets you flagged, audited, and tied up in compliance nightmares. Navina says do it at the point of care, with the patient in front of you and evidence tied to the chart, and you’ve solved two problems in one motion:
- the patient gets documented accurately and treated appropriately, and
- the record is audit-defensible by default.
This is the shift every risk-bearing organization is being pulled toward, like it or not. Prospective, encounter-linked documentation, replacing the year-end scramble.
The skeptic is the customer
Most incumbent risk-adjustment tools sold to the plan, where the budget lived and the value prop was obvious. Navina went after the provider, the harder door, and that became the moat.
Physicians are professional skeptics. You don’t win them with a prettier report. You win them by saving clicks and earning trust on accuracy, one patient at a time. Navina’s copilot pulls from everywhere a patient’s story lives (EHR, claims, HIEs, labs, meds, unstructured notes, scanned PDFs, and ambient) and reconciles it into one picture inside the EHR the physician already uses. No context-switching or separate screen (Privia executives have noted the importance of this). Suspected diagnoses and coding opportunities arrive tied to source evidence.
Navina’s core AI predates the LLM gold rush, homegrown and benchmarked hard back when accuracy wasn’t fashionable. Company data shows a 77% acceptance rate on AI-suggested diagnoses, against competitor case studies bragging about 40%. Twice the accuracy gets a physician to trust the next suggestion, which keeps them in the platform, which makes every downstream value-based workflow possible. Once a clinician is using Navina for a complete patient picture, risk capture and quality close natively instead of getting bolted on. Win the skeptic, let enterprise value follow.
Proof is in the adoption (literally) – Deploy something your clinicians will actually use!!
Let’s go to the numbers, starting with Privia Health, which works with 4,500+ providers across 1,140+ locations serving 5M+ patients. Its whole model is built on physician enablement, meaning they need to keep physicians happy and on platform to maximize their economics so… if a clinical AI tool holds up there, it holds up most places.
Privia’s rollout with Navina has been awesome. Within 6 weeks from contract to go-live, physicians trained in under an hour, 800+ clinicians onboarded in year one. What I’d circle is 87% weekly active users, holding steady as more clinicians piled on. Pretty cool when you have data to match your marketing material:
Privia physicians are also addressing 84% of Navina’s HCC suggestions, which is the risk-capture engine running inside the visit instead of in a March chart sweep. In Privia’s Georgia market, physicians cut chart-prep by up to 2.5 hours a day, and a clinical leader noted every doctor in one room said they’d pay for the tool out of pocket. Obviously the time saving is the qualitative measure while the HCC suggestion speaks for itself in terms of ROI.
Then there’s the independent study. A 2025 Phyx Primary Care Innovation Lab evaluation, run with the AAFP and notably not funded by Navina, studied 120 physicians across 19 practices using the copilot for 30+ days:
- 40% reduction in clinical review time on complex visits (10 minutes to 6)
- 32% drop in physician burnout (47% → 32%, significant at p=0.023)
- +0.153 average RAF lift across 3,100+ physicians
- +1.9 point STAR improvement across 32 quality measures
- 92% trusted the HCC suggestions; 94% found it easy to use
Zoom out to the full base (1,300+ clinics, 20,000+ clinicians, 3.5M+ lives) and Navina reports 49% more previously undocumented conditions identified, plus an 86% weekly active provider rate. In a category where most tools die on the vine after the pilot, that adoption figure is the tell.
Why health systems are circling
Health systems sat on the back end of VBC adoption for most of the value-based era. You can see it in their ACO performance. That’s changing, and the pressure runs two ways.
First, enforcement hits systems with MA exposure hard. When a large integrated system writes a high-dollar risk-adjustment settlement check, point-of-care documentation stops being a theoretical need. Tools that live in the workflow, where you physically can’t submit a condition that isn’t supported in front of you, are a better way to ensure compliance and solid documentation.
Second, there’s the EHR problem, and I’ll say what operators only say privately: EHRs solve for the lowest common denominator, and are not making ambulatory and primary-care documentation a top priority, because its incentives point at optimizing for the inpatient book of business. Any EHR solution is unlikely to be a tier-one AI vendor given their roadmap priorities.
In 2026, health systems want to move toward AI-native solutions, they’re tired of waiting on roadmaps they can’t bank on, and you can’t let a single dominant vendor get in the way of your end users and stakeholders – patients and physicians. Money lost under risk today doesn’t come back later.
The open question for Navina is whether it drifts toward clinical tooling or RCM, since those eventually pull on different resources. For now the roadmap follows two parallel tracks. One track keeps clinicians happy, because adoption is a fantastic talking point and wonderful moat for them in a sea of vendors. The second path continues its buildout of population health: risk stratification, quality, cost management, and prospective documentation integrity that automates audit defense before a denial lands.
What stays the same is the clinician in the loop, which is what separates Navina from competitors who are content to ship dashboards to a back office.
Taking action on point-of-care clinical AI
The infrastructure problem isn’t getting solved at the ecosystem level anytime soon (that would take a coordination miracle). But the lesson from Navina’s data is that you don’t have to wait for the system to fix itself. You can put the complete patient picture in front of the clinician, in the workflow, at the point of care, and let accurate documentation and better care fall out of that as a natural consequence.
Want to see what total patient context looks like inside your workflow? Talk to Navina.

