
Want to get these in your inbox to never miss an edition? Subscribe to Hospitalogy today!
Key Takeaways
Certificates of Public Need, or CONs, were created to control costs and centralize healthcare planning through state healthcare regulatory authorities.
CONs limit competition and prevent new capital and healthcare investments to enter old, established markets.
Health systems treat CONs as an asset and are encouraged to limit CON repeal, given that CONs create an artificial barrier to entry.
States are slowly repealing CONs. In cases like North Carolina, CON repeal may be replaced by Medicaid expansion.
The biggest losers from CON repeal will likely be small to mid-sized health systems.
What are CONs?
A CON is essentially a drivers license for healthcare services. The license permits you to operate that particular type of healthcare service in that particular certain state.
To complicate things just a bit more (because complication in healthcare is fun), each state has different CON restrictions and regulations. Some don’t have any at all.
CONs started as a federal program. In 1974, the U.S. mandated that states start regulating healthcare planning and development or they’d take away state federal funding. Then, in 1986, that CON mandate was repealed and several states dropped the regulation.
- Here’s a breakdown of CON laws by state. North Carolina, Hawaii, and DC are the strictest from a CON perspective, but it looks like North Carolina has notably made moves to repeal its CON in recent months.
For the most part, CONs exist to regulate larger, capital-intensive projects in healthcare like building new hospitals, surgery centers, or imaging facilities.
Some states are extremely strict and prevent pretty much every type of healthcare provider from building new facilities in their state without first going through the CON process.
Why do CONs exist?
States initially enacted CONs as a way to control healthcare costs. CONs are also a nifty way for states to increase access to care for charity patients, since most CON approvals come with a ball and chain of minimum required care for x% of indigent patients (a good thing).
- Right now, some level of CON regulation exists in 35 states. In 2019, Florida decided to repeal most of its CON moratorium. More on that later.
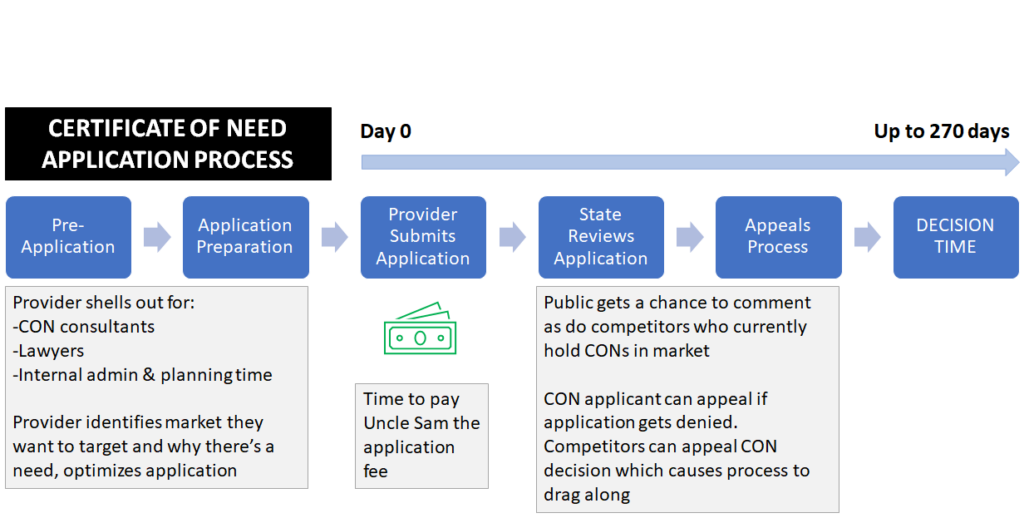
In order to be approved for a CON license, a healthcare provider has to prove that there’s a need for their particular service in the service area they’re targeting. To do so, the provider presents a case in the form of a CON application to that state’s health department showing key aspects of the project.
For instance, if I wanted to open up an inpatient rehab facility in North Carolina, I’d have to:
- Prove that there is a need for IRF beds in the market I’m trying to enter based on demographic trends or overall utilization per capita or whatever I can scrounge up. (States also publish need methodologies for companies to refer to during their application preparation)
- Provide the estimated capital outlay for the construction costs of the new IRF facility
- Ask for a certain number of IRF beds to be approved based on my claims above
At that point, I would submit my application to the state along with a payment for submitting.
Applying for a CON usually takes 9 or so months where providers overpay lawyers and suck up internal administrative time. And if the state denies the application? Add on another 3-6 months. Then you’re SOL from that point on until the state decides otherwise.
Join the thousands of healthcare professionals who read Hospitalogy
Subscribe to get expert analysis on healthcare M&A, strategy, finance, and markets.
No spam. Unsubscribe any time.
Why CONs suck.
CONs are anticompetitive and limit patient access. In a CON-controlled state environment, healthcare competition runs through the state. As a result, CON requirements become an unnecessary, artificial barrier to entry for every kind of healthcare provider.
This requirement results in fewer potential market competitors and hurts patient access. Studies have shown that CONs limit access to care in basically every service vertical. Not to mention any current CON holder can show up to hearings and appeal competitor CON applications.
- For the Select’s, Kindred’s, HCA’s, and other facility-based providers of the world, you’re losing out on major $$$ while you twiddle your thumbs waiting for project approval. Meanwhile, patients could be getting better access and better care at your brand new facility.
- Providers could somewhat circumvent the CON by partnering with local health systems who already own CONs, but JVs take a while, too and it’s sometimes hard to align if health systems aren’t prioritizing that specific vertical.
CONs are monopolies created by the state, and then perpetuated/controlled by existing CON licensees. They cost up to a few hundred thousand dollars to prepare an application, and they’re even considered an asset up to $1-2 million on the balance sheet of those lucky enough to own existing licenses – usually hospitals.
These states aren’t running competitive, free markets. While they might be trying to control costs, quality suffers and monopolies thrive, which I personally hate.
- Think about it this way: state data might show that there are ample diagnostic imaging centers to get a CT scan completed, but what that data doesn’t show you is the imaging center operating in a run-down shitty facility with a 20-year old, poorly maintained CT.
I look at it like this: You can either have more competition and more choice for patients, or less…and maybe save a buck or two. I choose the competitive option.
Progress on CON Repeal.
Even though some level of CONs exist in 35 states, policymakers are making a push to change that. I think they also got their shit together after realizing they had no bed capacity during the pandemic caused by – ahem, you got it – CON laws denying hospital bed applications.
24 states altered CON laws during the pandemic. Montana repealed all CONs except for long-term care, and it seems as if Georgia is getting close to repealing or modifying its regulations.
- Several other states are considering serious CON repeals as well. Washington extended the suspension of its CON thru 2023, and Tennessee greatly loosened CON application requirements and eligibility criteria. Same with North Carolina, which recently loosened the capital requirement associated with a CON application and may be looking to do more soon.
CON repeal can take a bit of time since the players who hold the CONs typically lobby or argue against the legislation.
Think about it – you have a million dollar asset on your balance sheet. Strategically, would you want it to vanish into thin air WHILE introducing yourself to competition? Over time, though, state policymakers will get to the right decision here and repeal most state CON requirements.
- Let’s touch on a state that recently lifted a portion of its CON: Florida.
Case Study: Florida
Back in mid 2019, Florida lifted CON requirements on every type of healthcare facility save for nursing homes (SNFs), hospice agencies, and intermediate care facilities.
The change created a TON of healthcare activity in Florida.
Let’s look at the impact on inpatient rehabilitation facilities, for instance.
- 14 operators have plans to either open up new IRFs state-wide or expand the capacity of their current facilities, and the state will benefit from an estimated 800 new IRF beds and the external effects from that bed expansion: construction & development investment, more healthcare jobs, and better patient access and care for an aging Florida population HEAVILY skewed toward Medicare & Medicare Advantage.
- Of Encompass Health’s next 25 planned sites (page 30), nine (almost 40%) are located in Florida.
If the private sector thinks there’s THAT big of an opportunity for business in a sector as stable as INPATIENT REHABILITATION, that meant Florida was way behind in IRF access. It makes you wonder what would happen if states nationwide dropped their CON requirements.
The positives of expanded patient access, increased investment and business development, and job creation vastly outweighs the potential for more state healthcare costs in my mind.
Bottom line: let’s repeal some CONs, folks.
Resources:
- For you crazies who want to do more research – this is a well-informed article from U.S. News. (Link)
- How CON laws affect quality and access – Mercatus. (Link)
Want to get these in your inbox to never miss an edition? Subscribe to Hospitalogy today!